Department of Otolaryngology, Head and Neck Surgery
|
Otology Department of Otolaryngology, Head and Neck Surgery |
| Home | Unit One | Unit Two | Unit Three | Unit Four | Unit Five | Unit Six | Unit Seven | Unit Eight | References |
The normal external ear canal, middle ear, and Eustachian tube anatomy are reviewed within this section.
Estimated time to complete: X minutes. Please complete the entire unit in one access period.
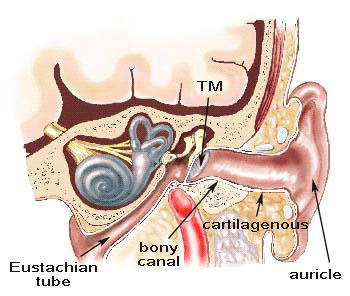
The External EarThe external ear begins laterally with the auricle of the ear and proceeds medially through the external auditory canal to the tympanic membrane (TM). The outer portion of the canal is an extension of firmly attached cartilage from the auricle. The squamous epithelium is loose and continuous with that of the face as it contains numerous hair follicles, sebaceous, and ceruminous glands. Tympanic and squamous portions of temporal bone surround the inner portion of the canal. The canal curves anteriorly and inferiorly before it narrows. The adult external meatus is approximately 3.5 cm in length. The skin surrounding the temporal bone is tightly attached. Being the only skin lined cul-de-sac in the body, this canal has developed a self-cleaning action allowing migration of keratin from the drum outward, slowing as it reaches the outer wall of the canal. |
|
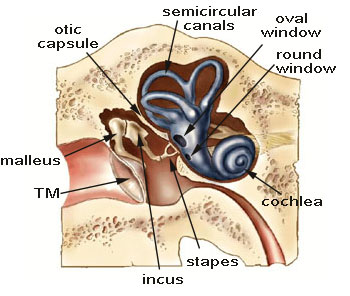 The Middle EarThe middle ear is the space between the tympanic membrane and the bony otic capsule of the inner ear. It includes the ossicles, muscles, Eustachian tube, and facial nerve. The middle ear space contains the incus and malleus, the stapes, the oval and round windows of the cochlea. The auditory ossicles transmit mechanical energy in the form of vibrations to the endolymphatic fluid within the cochlea. The malleus and incus work as one as they interact with the stapes. The stapes is shaped like a stirrup. The oval window houses the footplate of the stapes. The stapes with its footplate transmits sound through the oval window. The stapes moves in a rocking motion that sets the inner ear fluid in motion stimulating the hair cells to eventually detect the sound. The round window is a thin membrane that closes the cochlea allowing the fluid to move. The middle ear includes two muscles, the tensor tympani and stapedius muscle. The tensor tympani muscle arises with a tendon extending to the handle of the malleus. This muscle causes the tympanic membrane to pull inward. The stapedius muscle, innervated by the VII cranial nerve, pulls the stapes posteriorly. This action attenuates the sound transmission and increases the resonance and frequency of the ossicular chain. This can be tested by the stapedial reflex test. |
|
The Tympanic Membrane |
|
|  |
Right eardrum | Left eardrum |
| The anterior canal wall is relatively vertical and obstructs the view of the anterior TM in many patients.The
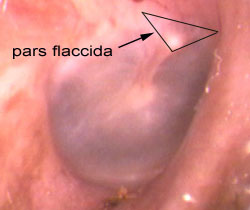
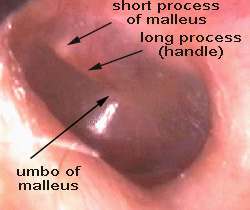
posterior canal wall is rounded so that the posterior tympanic membrane is easy to see. Notice the long process of the malleus(also called the manubrium or handle) in the middle of the TM. The tympanic membrane separates the external and middle ear compartments. It attaches to the malleus handle. The oval- shaped membrane is situated at a 55-degree angle. The 9-10mm maximum diameter is measured posterosuperior to anteroinferior. The membrane is concave toward the ear canal. The tympanic membrane’s conical shape results in a light reflex from the umbo (most inferior portion of the malleus) projecting anteroinferiorly.The normal TM may not have a light reflex if the light is at an angle as in the right ear. Its anterior portion is angled medially; posterior portion is angled laterally. The tympanic membrane is thin and semi-transparent with a pearly, gray appearance. It is composed of three layers: An outer, epithelial (ectodermal)layer; a middle, fibrous layer; and an inner, mucosal(endodermal) layer that is continuous with the squamous lining of the middle ear cavity. The fibrous layer is composed of circumferential and radial fibers that provide shape and consistency to the eardrum. The radial fibers allow the conical shape. The circumferential fibers provide strength while allowing the transmission of the vibratory energy. The portion of the tympanic membrane that contains radially oriented fibers is the pars tensa and the portion without is the thinner pars flaccida superiorly. The appearance is judged on color, vascularization, landmarks, discharge, and physical orientation. The most prominate landmark on the tympanic membrane is the malleus handle. The pars tensa forms the majority of the membrane with the pars flaccida in a triangular shape superiorly. |
|
The Eustachian TubeThe Eustachian tube is an outgrowth of the nasopharynx. The lining contains many mucous glands. The cartilagenous portion is about 2/3 the length beginning at the pharyngeal end. The ear portion is bony. The tensor veli palatini, innervated by the V cranial nerve. When it is contracted, it opens the cartilagenous portion during swallowing. At birth the tube is 17-18 mm in length that grows to 35-36 mm by adulthood. It is situated at an angle of 45 degrees with the horizontal. The interior is lined with a mucosal surface comprised of pseudostratified ciliated columnar epithelium that is continuous with the nasopharynx extending into the middle ear. The Eustachian tube is normally closed and opens during yawning and swallowing. In these times, the middle ear is susceptible to organisms from the nasopharynx. The cilia and mucous secretory enzymes help keep the middle ear free from disease. The Eustachian tube equilibrates air pressure, protects the middle ear from nasopharyngeal sound pressure and secretions, and drains the middle ear secretions into the nasopharynx. Dysfunction can occur in three ways:
|
|
| Home | Unit One | Unit Two | Unit Three | Unit Four | Unit Five | Unit Six | Unit Seven | Unit Eight | References |
Site administrator:
Barbara
Heywood MD.
Copyright © 2014
 All rights reserved.
All rights reserved.